


















































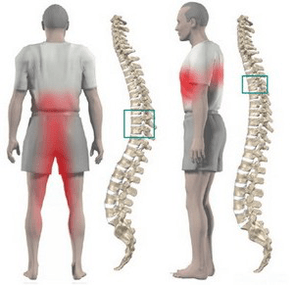
In the case of thoracic osteochondrosis, organs associated with the spinal cord area, located at the level of the affected thoracic area and down, often suffer. Violation of the normal activity of the spine leads to immobility of the arms, legs and body as a whole, dysfunction of the pelvic organs, respiratory muscles and internal organs.
Osteochondrosis is a degenerative-dystrophic disease of the spine, which is based on changes in the intervertebral disc with involvement in the pathological processes of neighboring vertebrae and intervertebral joints with the rest of the ligament apparatus.
Anatomical features of the spine
The mobility and stability, elasticity and resilience of the spine largely depend on the intervertebral disc, which is one type of cartilage connection between bones and provides a strong bond between neighboring vertebral bodies. The total length of the intervertebral disc is a quarter of the length of the spinal column.
The most important function of the disc is to reduce the vertical load on the vertebrae. The disc consists of three parts:
- hyaline plate (closely adjacent to vertebrae);
- nucleus pulposus (filling the gap between plates);
- fibrous ring (surrounding the nucleus from the outside).
The nucleus contains cartilage cells, closely intertwined collagen fibers and chondrines (proteoglycans). The anterior surface of the disc is covered by the anterior longitudinal ligament, which joins closely to the vertebrae and independently reverses the disc. The posterior longitudinal ligament joins strongly with the disc surface and forms the anterior wall of the spinal canal. The intervertebral disc does not have its own blood supply, so it consumes material that comes through diffusion from the vertebral body.
The vertical load distribution in the spinal space occurs due to the elastic properties of the disc. As a result of the pressure, the nucleus pulposus expands, and the pressure is redistributed to the fibrosus annulus and hyaline plate. During movement, the core moves in the opposite direction: when bent - in the convex direction, when not bent - forward. When the spine moves, muscles, ligaments and discs are put into work. Thus, a violation in one link leads to a violation in the entire kinetic chain.
Causes and mechanisms of disease progression
In the development of osteochondrosis, a special role is played by mechanical effects on the spine. Under the influence of unfavorable static and dynamic loads, the nucleus pulposus gradually loses its elastic properties (due to polysaccharide depolymerization), forming protrusions and sequesters.
The process of disc degeneration is influenced by genetic predisposition, which leads to the development of changes in the posterior neuromuscular apparatus, changes in the structure of glycosamine, and violation of the distribution of collagen fibers in the disc. Genetic factors are most important in the occurrence of thoracic osteochondrosis, subject to increased functional activity.
Risk factors for the development of degenerative changes in the spine include anatomical features of the disc, which is an evolutionary imperfection. One of these features is the structural nutritional feature. In the human body, discs are made up of tissues that do not diffuse well. Closure of blood vessels already occurs in childhood. After feeding occurs due to the diffusion of material through the end plate.
Nutrient penetration stimulants are dosing loads that exclude static posture and great stress. Physical inactivity is one of the major risk factors for thoracic osteochondrosis. Therefore, regular exercise is an important preventative measure.
The peculiarity of the microscopic structure - some cells - reduces the intensity of the regenerative capacity and the rate of recovery of the disc components. Anatomical features are the weakness and lack of strength of the disc in the back. This contributes to the appearance of wedge -shaped discs in the lower part of the thorax and lumbar region.
Great importance in the development of osteochondrosis is given to involuntary changes. Degenerative changes actively begin to increase after 30 years. The synthesis of components required for discs (glycosaminoglycans) continues, but their quality is deteriorating. Hydrophilicity decreases, fibrousness increases, sclerosis appears.
Stages of intervertebral disc degeneration:
- prolonged asymptomatic course, degenerative changes in the intradiscal component, displacement of the nucleus in the disc;
- obvious radicular symptoms of thoracic osteochondrosis, spinal cord compression, protrusion of the nucleus pulposus (protrusion, 1 degree);
- disc rupture with protrusion of hernia (hernia, 2nd degree);
- degenerative changes in the extradiscal component (grade 3).
Pathological protrusion compresses nerve roots, blood vessels or spinal cord at various levels (cervical, thoracic, lumbar), which determines the clinical picture.
Restriction of mobility in the thoracic spine, caused by the presence of the chest, contributes to the least trauma to the intervertebral disc, and therefore osteochondrosis. Physiological thoracic kyphosis contributes to the redistribution of weight of the upper half of the body to the lateral and anterior parts of the vertebrae. Thus, intervertebral hernias and osteophytes form on the anterior and lateral surfaces of the spinal column. Osteophytes and posterior hernias are extremely rare.
Osteochondrosis contributes to narrowing of the intervertebral foramina and compression of spinal cord roots and sympathetic fibers. Sympathetic fibers originate from the gray matter of the spinal cord, then gather into nodes, from which they are transmitted to all internal organs. This leads to the fact that thoracic osteochondrosis, in addition to typical neurological disorders, leads to dysfunction of internal organs (vegetative, vasomotor, trophic) and artificial somatic diseases. This characteristic of thoracic disc osteochondrosis explains the difficulty in diagnosing and prescribing proper treatment.
Symptoms of thoracic osteochondrosis
Thoracic osteochondrosis is more typical for people with an inactive lifestyle. At the same time, there is no stimulating effect of dosing load on the spine, which contributes to the disruption of disc recovery. The disease develops in people who work at computers for long periods of time, hunched over, etc. such people need to independently perform therapeutic exercises.
Often, chest osteochondrosis is indicated by dull aches, less frequent aches and burns. The pain is localized between the shoulder blades. The patient is disturbed by the feeling of chest compression. Upon feeling the spinous process of the thoracic vertebrae, local pain is detected, which increases with axial load on the spine, deep inspiration and body rotation.
Some patients experience sharp pain in the scapula and lower chest (posterior costal syndrome). This symptomatology develops as a result of lower rib displacement. The pain increases sharply when turning the body. More often, the pain syndrome disappears suddenly.
Often the pain in the chest becomes a belt, corresponding to the travel of the intercostal nerve. Sensitivity in the conservation zone of the corresponding nerve endings is disturbed, paresthesia appears, and there is often a shallow and deep decrease in sensitivity. Possible violation of abdominal compression function, changes in the reflexes of the knee and calcaneal tendons.
Violation of the function of internal organs occurs when any nerve root is compressed at a level from 1 to 12 of the chest. In the thoracic region there are structures responsible for the preservation of the lungs, heart, intestines, liver, pancreas, and kidneys. Therefore, there are no hallmarks only for thoracic osteochondrosis.
The disease is indicated by symptoms of other pathological features:
- hard to breath;
- intense night pain;
- "heart", angina pain;
- pain in the mammary glands;
- pain in the right or left hypochondrium (symptoms of cholecystitis and pancreatitis);
- pain in the throat and esophagus;
- pain in the epigastrium, stomach (symptoms of gastritis, enteritis and colitis);
- sexual dysfunction.
Diagnostics
The greatest value in the diagnosis of thoracic osteochondrosis has a chest X-ray examination. The picture shows a decrease in the height of the intervertebral disc, sclerosis of the end plate, the formation of osteophytes.
Computed tomography allows you to describe the condition of the vertebrae, spinal joints, the size of the spinal canal, determine the location of the hernia protrusion and its size.
When carrying out a differential diagnosis, it is necessary to carefully collect anamnesis and compare all the clinical signs of thoracic osteochondrosis with the symptoms of other diseases. For example: pain in the heart with osteochondrosis is not stopped by nitroglycerin, epigastric pain is not associated with food intake, is not seasonal, all symptoms appear mainly in the evening and disappear completely after night rest.
How to treat thoracic osteochondrosis?
Treatment of osteochondrosis of the thoracic spine in almost all cases is conservative. The indication for therapy is the predominance of visceral syndrome with neurological disorders. Primary orthopedic treatment should be adequate spinal traction:
- active vertical gravity underwater;
- passive horizontal traction in an inclined bed using a Glisson loop in the event of damage at levels 1-4 of the thoracic vertebrae, by the axillary cord in the event of damage at levels 4-12 of the thoracic vertebrae.
Drug treatment consists of performing paravertebral blockade with novocaine solution. With exacerbation of the disease, analgesics and sedatives are used. With unspecified pain syndrome, it is permissible to use ointments with analgesics and anti-inflammatory drugs at home.
After elimination of the acute phenomenon, massage of the back and lower extremities muscles is used. Manual therapy is indicated for 1-3 degrees of osteochondrosis in case of development of functional restriction. It includes a variety of options for soft and rough effects on the back muscles.
Therapeutic exercises allow you to load all parts of the spine in a dosage way, which stimulates the recovery process. An important condition for exercise therapy for osteochondrosis is to exclude vertical loads.
Physiotherapy: UHF treatment, ultrasound, inductothermy, radon and pine-conifer salt baths. At the spa level, underwater attractions and hydromassage are actively used.
Surgical treatment is rarely used. The indication for surgical intervention is compression of the spinal cord by prolapsed disc fragments.